The main issues and challenges of this difficult revision rhinoplasty begin with an explicit open roof deformity, noticeable like few other cases due to the dorsal transparency, forming a typical combination of wide gap between nasal bones, visible ridges at its sides, flat dorsum which is also poorly or undefined; this was caused by failing to perform the required osteotomies which are mandatory after hump removal, leading thus in this case a fully blown typical tetrad of deformities.
Like a chain reaction cascade, every and each revision rhinoplasty scenario due to failing to perform competent osteotomies, such an important maneuver, lead to a tetrad of associated issues in a higher or lesser grade depending on the quality of the nasal tissues, which are the open roof deformity, a broad nasal pyramid with broad base, the inverted V deformity and a pinched middle vault.
The nasal wall is formed by a rigid and solid upper part made by the nasal bones, plus a lower part formed by the upper lateral cartilages which are soft; in absence of competent osteotomies or infractures of the nasal bones after shaving the hump, performing paramedial bone resections or both, the osseous walls stand their position leaving a gap between them at the dorsum, which is the so called open roof, being its closure accomplished by the aforementioned osteotomies; such separation between bones lead to a broad or square flat dorsum without any suitable definition and visible side ridges, the lower or larger the hump resection the more undefined and wide the dorsum is and the more open the roof becomes.
As may sound evident, failing to perform osteotomies leads to a broad nasal base and a broad pyramid or, should this be an asymmetrical failure, a lopsided pyramid or asymmetric one.
Subsequently to the missing osteotomies, when the surgeon, unaware of his actions, pushes the lateral walls of the pyramid to the midline, then the cartilaginous walls made by the upper lateral cartilages lean medially due to the natural hinge they have at their maxillary stand, whilst the bony wall nasal bones remain solidary to the maxilla and stay firm in place, thus due this uneven closure of the nasal walls the lower pyramid upper lateral cartilages dissociate and dislocate from the upper pyramid nasal bones leading to a visible inverted V, being such V ridge the lower edges of the nasal bones and the gap between them and inwardly dislocated upper lateral cartilages which separate from the former.
The formerly described phenomenon allows closure of the open roof only at the lower and soft part, not at the upper hard one where the open roof deformity stays, and in between the two halves, hard and soft, of the pyramid a ridge of separation between bones and cartilages is created, however the upper lateral cartilages not only lean towards the midline cartilaginous septum but also do collapse beneath the dorsum level and pinch the middle vault because the fail to receive the support of the normally solidary nasal bones and end in a free fall only supported by the weak mucosa lining of the airway, being such pinched middle vault a visible deformity and in many cases also a functional breathing impairment.
In an ideal scenario there should exist an en bloc displacement of the entire nasal pyramid walls to the midline to prevent the tetrad of deformities, and for this goal the infracture osteotomies are essential to allow the nasal bones free float in parallel with and synchrony with the upper lateral cartilages, without any dissociation and therefore without any kind of deformity, achieving total roof closure and good stability of the pyramid, with or without other additional maneuvers in selected indications.
A maneuver of such paramount importance like the nasal bones osteotomies is a very basic and simple one, of low difficulty indeed, being very hard to understand and even more difficult to justify why some surgeons still fail to execute it when, in all the medical literature, is considered as mandatory whenever a nasal pyramid dorsum gap is created; since Dr. Joseph and disciples' invention of the basic rhinoplasty technique and the specific surgical instruments for its execution in the first decade of 20th century, the surgeons know that osteotomies are a must, in spite performing them brings swelling and bruising to patients and require specific surgical training and good skills to avoid accidents; surgeons face and assume risks to achieve safe and successful rhinoplasties, that is their work; whoever does not feel ready to perform osteotomies in noses should not carry out any single rhinoplasty in his career.
Treatment of the tetrad of deformities due to missing or incompetent osteotomies begins with something as obvious and easy as performing proper and competent osteotomies, since this will close the open roof, will redefine the dorsum, make it narrow, get rid of the ridges and narrow the nasal base and the pyramid; to correct the collapsed upper lateral cartilages, the inverted V deformity and the pinched middle vault there exist two options; whenever it is possible a direct suture of the upper lateral cartilages to the cartilaginous septum may suffice in non mutilated cases which not too pinched which did not receive the deformity long ago; otherwise spacer or spreader grafts are bound to be used, well planned, very thin to prevent thick dorsums and sutured in place to prevent their migration, displacement or visibility; may the skin be very thin and allow visibility of the work done on the dorsum then a temporalis fascia graft has to be used to camouflage the dorsum and make it look neat and smooth.
This case is a paradigm of all the former, the complete tetrad of cascading deformities due to such an avoidable cause as failing to perform osteotomies of the nasal bones after removing the dorsal hump.
There are other three visually evident issues in this nose plus another which, as mentioned at the beginning, is undetectable externally but was discovered during the surgical direct visualization; another perfect reason why open approach access is absolutely mandatory in revision rhinoplasties.
This nose received total or subtotal resection and damage of the lateral cruras of the alar cartilages, the domes of the tip and pinching of the nose and the nasal valve; this is the external diagnosis by such typical and obviously pinched look of the tip, the tip bossing and the too sharp tip shape; intraoperatively this diagnosis was confirmed and expanded, since both tip domes had been mutilated, severed and the lateral cruras subtotally resected and the remains damaged beyond repair; all this makes a real write off for the tip, columella and alae, which required total rebuild with newly made handicraft elements.
Also externally visible and palpable there was a oversized, too long and over prominent strut graft between the medial cruras of the columella, which probably was not initially indicated or, should it have been, its calibration was poor; this strut graft made a hearable clicking when the patient spoke or chewed, something very annoying, and lead to a Pinocchio nose due to the over projection of the tip; this issue was intraoperatively confirmed.
Somehow clearly it can be seen the tip is upturned with an excessive nasolabial angle or angle between columella and the horizontal plane crossing the upper lip; the nostril rims were totally collapsed and unsupported; probably due to the damage to the lateral cruras.
Finally, one unforeseeable and preoperatively undetectable issue was the soft dorsum, this means the lower half, was over resected into a saddle nose deformity; however this hollow loss of substance was not visible externally because the missing dorsum was replaced and the profile stood by a mass of fibrotic tissue; this fibrosis has, necessarily, to be removed in every and each revision rhinoplasty, so in an ordeal of unexpected complexity the correction of a saddle nose deformity was added to the surgical plan; additional problem, the septal cartilage was not available for graft harvesting since it was previously touched to build the strut graft.
After thorough debridement or removal of fibrosis and non viable structures, both ear concha bowls were used as donor site for the grafting required in this case; after trimming down the excessive columellar strut an extended tip and columella entire grafting with meticulous scoring was used to either rebuild the tip, lower the nasolabial angle, derotate the tip and shape the wished new tip domes; two handmade new lateral cruras were applied and repositioned to provide support to alae, nostril rims and nasal valve, in order to correct the pinching too; two spacer or spreader grafts were sutured between the upper lateral cartilages and the soft septum to treat the pinching at the middle vault and the inverted V deformities; of course complete and proper osteotomies were applied; finally an onlay dorsal graft was tailored and applied with suturing to restore the right dorsum level which was sunken due to over resection.
The brilliant and natural final result allows full restoration of a harmonious and feminine nose, no evidence or trace of any of the initial deformities, no signs suspicious of having underwent two previous rhinoplasties and with a well balanced, supported, functional and suitable in shape and size nose.
READ LESS






 Sending vote...
Sending vote...

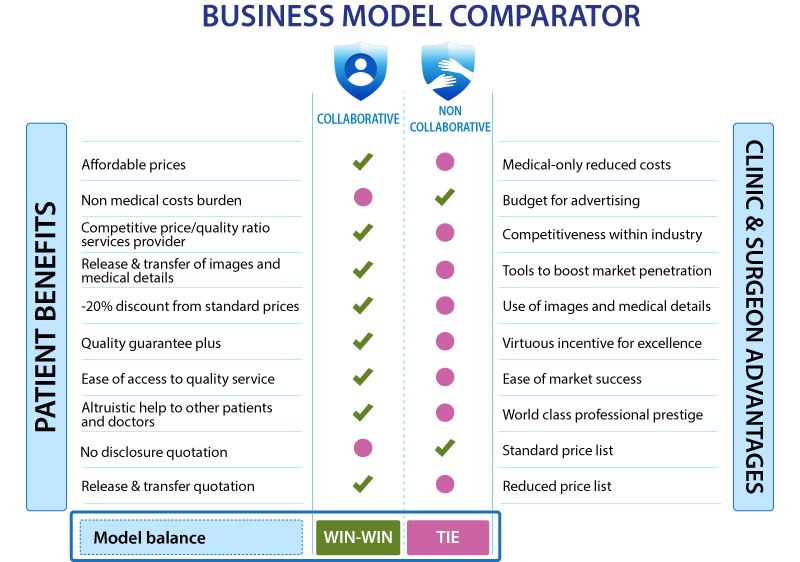
 READ MORE ABOUT BENEFITS OF THE COLLABORATIVE MODEL
READ MORE ABOUT BENEFITS OF THE COLLABORATIVE MODEL
 +34-900-838448
+34-900-838448 +44-0-800-0488400
+44-0-800-0488400 +1-844-4000840
+1-844-4000840





























