Post large volume pregnancy abdomen in which is seen an atypical combination of minimal skin excess, normally a large apron of skin is present, plus a extreme weakness of the muscles, larger than the usual situation in tummy tucks, due to a severe diastasis recti at the linea alba or abdominal tendon of the midline; notwithstanding there is moderate excess of cutaneous cover, much more after the reduction of the abdominal girdle incompetence which indirectly increases the amount of spare skin; both issues are optimal candidates for an abdominoplasty.





 Sending vote... Sending vote...
Sending vote... Sending vote...

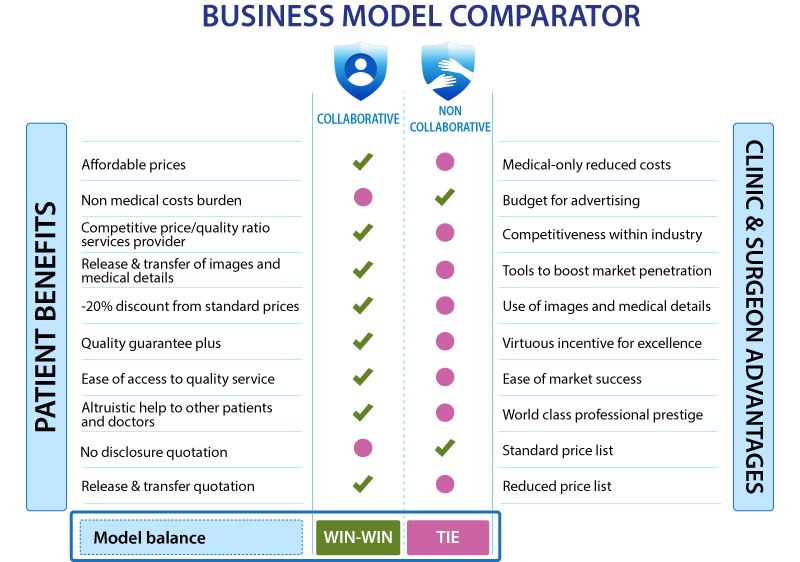
 READ MORE ABOUT BENEFITS OF THE COLLABORATIVE MODEL
READ MORE ABOUT BENEFITS OF THE COLLABORATIVE MODEL
Due to the competitiveness scenario of the markets most plastic surgery clinics and plastic surgeons feel forced to invest large sums of money into advertising and marketing campaigns; this non medical additional cost is always and necessarily charged on top of the final price paid by patients, leading thus to an overprice of surgeries and treatments. No one patient wishes to bear that financial burden embedded in the surgical costs, furthermore neither surgeons nor clinics are happy to increase their retail prices and penalize their customers with costs not bringing any kind of special medical benefit, safety enhancements or results improvement; the promotion budget aims only to disseminate the public knowledge of a services provider and raise the awareness about its presence to potential customers, but not to make the service or the product a better one.
Seems like this model is a no-way-out labyrinth from which no one can be freed, furthermore it is such a tempting, easy and hassle-free way that actually most patients and plastic surgery providers are locked into it, happily or with resignation, paying a high price due to being non collaborative; however there is an ideal alternative, based on keeping up a good hard work based on a strive for providing quality service and achieving patients' satisfaction, which necessarily requires the decided support of the clients and somehow their involvement in such virtuous business model grounded on top-notch results
Print screen alert
You attempted an unauthorized action. All contents of this site are private and protected. Print screen are not allowed. We have reported with your data location to prevent any ilegal action against the protected contents of this website.
 +34-900-838448
+34-900-838448 +44-0-800-0488400
+44-0-800-0488400 +1-844-4000840
+1-844-4000840

































