The high location of the belly button plus a practically nonexistent excess of skin at the upper abdominal area make impossible including the original belly button hole within the skin of island which is to be removed, forcing to add a mini vertical scar above the long horizontal one.
Note that the belly button itself can't be mobilized or relocated, not even surgically, since it is like a funnel of abdominal skin firmly attached to the muscular wall, however the location at the abdominal pannus through which the belly button surfaces behaves like a hole around a button of a shirt during the abdominoplasty; the belly button is a solid attachment impeding the mobilization and extension of the anterior abdominal pannus or cloth, so its release is mandatory in tummy tucks by means of a circumferential incision at the edge of the navel, outlining and creating the naturally born original hole of the belly button; the surgical tightening and sliding downwards of the abdominal skin makes the original hole of the belly button lay within the portion of skin to be cut away and discarded; then a new hole is practiced exactly above the belly button location to allow its surfacing through a new skin perimeter but at the same location; should the patient have an abnormally too high belly button location, a poor excess of spare skin at the upper abdomen or both, then the cloth downwards extension is not sufficient to allow the original hole of the belly button be included within the island of skin removed, ending such old hole somewhere between the new surgically practiced hole at the belly button location and the suprapubical horizontal incision, requiring closure of such redundant hole in a vertical fashion with a short vertical scar, like can be seen in this case, plus the typical and standard long horizontal suprapubical incision between hips along the natural crease formed between abdomen above and pubis and groins below, and the also typical and standard small circumferential incision around the belly button.
In other words, the belly button behaves as a real buttoning of the abdominal cloth and this has to be released to allow proper tightening and adjustment of the anterior abdominal skin; to do so an incision is made surrounding the funnel of the navel which leaves a hole, and this hole is mobilized downwardly during the abdominoplasty cutaneous vertical tightening down to a point of perfect skin adjustment of the anterior abdominal skin; a newly made surgical hole is practiced above the belly button through which it is extracted and sutured to the new surrounding surface; the original hole is cut away and discarded within the block of skin deemed as excess of pannus; should the hole not lay within the removed skin then it has, necessarily, to be closed in a vertical fashion; failing to do the latter in the suitable indications would entail a certain risk of bad scarring, catastrophic necrosis or distortions of the pubic anatomy like excessive upwards migration of the hairy pubis; to set things clear, the amount of skin which can be cut away is non negotiable whatever it takes or the consequences are, removing too little leads to persistent deformities and removing too much causes complications, wound closure has to be performed to the perfect point of tension.
Actually, this abdominoplasty case would have been a shoehorned indication if skin excess had been the only motivation; this abdomen has a primary issue which is the muscular weakness and, as can be seen in the results, the reinforcement of the abdominal girdle is absolute, returning to the original tendinous firmness; abdominal workouts would never achieve such outcome since the problem is not strictly muscular but of tendon widening, being the only option its surgical treatment.
Scars are always a serious drawback and need to be seriously considered before moving forward to any kind of abdominoplasty; only cases with major deformity like this one are reasonable candidates to a procedure which will likely pay off for such unsightly scars; notwithstanding the final decision is always on patient's side, after a more than necessary thorough reflection about the pros and cons received from a tummy tuck.
Very important note: the odd ordinal number before and after results images shown are taken with the patient in a relaxed attitude, no muscular contraction is exercised and the abdomen is totally loose without active support from the muscles; no instruction was given to the patient to actively push in her abdomen, the results are as trustworthy as depicted here; to the contrary the even ordinal number before and after results images shown are taken instructing the patient to perform her maximum push in abdominal contraction; the final result is so brilliant that the postoperative relaxed look is flatter, firmer and widely superior than the maximum abdominal push in contraction preoperative one.
READ LESS










 Sending vote...
Sending vote...

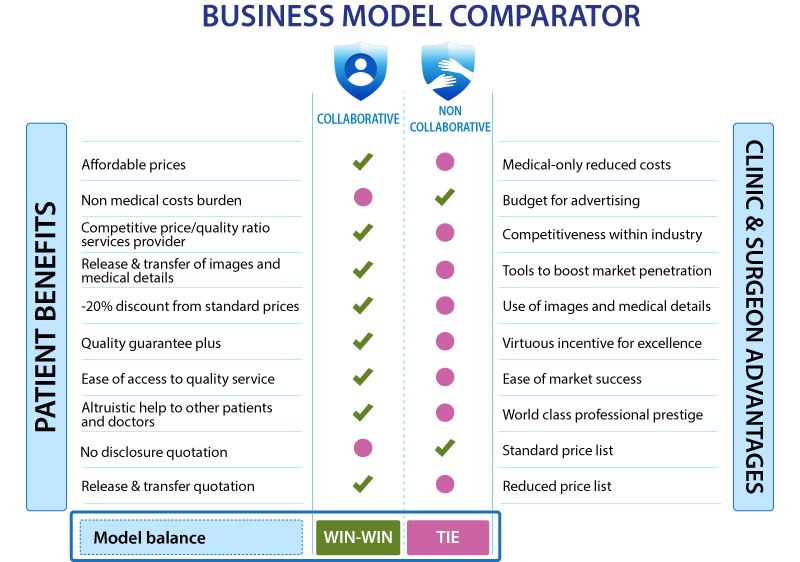
 READ MORE ABOUT BENEFITS OF THE COLLABORATIVE MODEL
READ MORE ABOUT BENEFITS OF THE COLLABORATIVE MODEL
 +34-900-838448
+34-900-838448 +44-0-800-0488400
+44-0-800-0488400 +1-844-4000840
+1-844-4000840

































