This website uses its own and third party cookies to provide a better service. If you continue to browse, you are deemed to have accepted their use. See our Cookies Policy and Legal Notice and Terms of Service
Very difficult breast implants revision case of extremely high complexity on a patient who, due to a digestive nutritional disorder which caused her poor healing ability, suffered of null adhesion of breast implants to the surrounding tissues and thus failed to form attachment to the ribcage in spite the implants were of top quality and well textured; this, associated to a very weak cutaneous and glandular cover, lead to a bottoming out downwards dislocation displacement of the prostheses and significant grade of tenting close to be a full symmastia.
READ
Essentially there coexist two problems of breast implants pocket definition; on one side the pocket was over expanded at the lower pole due to the bottoming out of the implants and the poor firmness quality of the patient's breast, and on the other side the implants, especially the left one, moved towards and expanded the inner cleavage of the breasts, creating a tenting effect which in some positions or with the brassiere on allowed rubbing of implants in symmastia.
As a direct and evident consequence of the former the implants did lose their centricity according to the nipple areola complex, becoming largely eccentric inwards and downwards; this can be clearly noticed by the landmark inframammary scars belonging to the first intervention; also the nipples were pointing up and laterally, which is exactly to the opposite direction of the migration of the implants, since inwards migration or symmastia entails outwards nipple orientation and the downwards bottoming out leads to star gazing nipples.
Due to the aforementioned phenomena there is a problematic over dissection and over growth of skin at the lower and medial poles of the breasts, which need to be reattached to the ribcage, being the perfect candidate for a multipoint capsulorrhaphy which allows both redefinition of the prosthetic pockets and eradication of the over expanded excess of skin; due to the particularities of the case and in order to prevent a new failure of adhesion, the patient opted for polyurethane coated implants which provide the highest grade of tissue adhesion from them all in the market thanks to their bio velcro effect, anatomical shaped and cohesive gel filled, significantly larger than the previous ones due to express patient request.
These revision capsulorrhaphies and other revisional techniques have to be performed via areolar approach to obtain full visualization and complete access within the breast pocket; however this patient had a previous inframammary incision so she was offered two options, which were new areolar incision or extending the already existing inframammary scar to allow safe performance of the revisional procedure, opting for the second one in spite the scars lengthening.
The capsulorrhaphy entailed a vertical row of anchors at the inner side of the pocket to redefine the cleavage from the 3rd to the 6th rib arcs and another horizontal row of anchor sutures redefining the submammary crease; anchors are separated between them 10 to maximum 15 mm, otherwise they could fail or leave hammock effects between their gaps.
The combination of the multipoint capsulorrhaphy and the highly adhesive polyurethane coated implants lead to an impressive result, full correction of cleavage tenting and symmastia, no recurrence of the bottoming out and perfect centricity of implants beneath the nipple areola complex, without any kind of nipple orientation distortion.
READ LESS
RATE THIS CASE FOR THE COMMUNITY
How much did you like the case?
Sending vote...
How much has been useful to you?
Sending vote...
Ranking
Usefulness
Popularity
CURRENT PRICES QUOTATION FOR THIS CASE
Choose body area and select your products purchase
This information is indicative only and does not represent an obligation with patients or a prediction of forthcoming events, since is based on statistical means for large groups of patients, with the variability that implies, and the biased experience of medical professionals.
Medicine and Surgery are not exact sciences, therefore it is not possible to foretell the most likely evolution neither establish the most suitable management for each individual case until the moment the physicians can preoperatively evaluate the patient and receive feedback about the postoperative.
One surgical process can't be fully predictable or be rigidly scheduled on a previous protocol, so the management plan may be modified at any time based on the requirements that could be considered as necessary or most suitable.
Healing is an imprecise and always unpredictable process due to the uniqueness nature of each patient; even with your physician prioritising post-op patient care excellence and scar minimisation techniques and treatments your evolution and results may be likely different to the information contained on this website, therefore your physician cannot guarantee any specific scenario and outcome commitment regarding your procedures.
Remember that all surgery is likely to produce lasting swelling and a lifetime permanent scar, which is likely to partially evolve over approximately 12 to 18 months or longer because this is an issue of unpredictable kind; some patients may be prone to permanent swelling and bad scarring.
Information on our website is not a substitute for a personalised, individual consultation that includes a physical examination, history taking, a discussion of the potential risks including potential common complications, pros and cons of various procedural options, and the likely outcome expectations of your surgical procedure. Only an in-person consultation and examination can help your physician to provide you with information about what you, personally, as a unique individual, can expect.
Dr. Alejandro Nogueira's opinions, indications, procedures, techniques and methods of diagnosis, treatment and management change frequently as new information is available due to scientific knowledge and state-of-the-art medical practice progress; we aim to keep information updated, but it is possible that some information may have been superseded and is in process of being added to our website, therefore it may not represent Dr. Alejandro Nogueira's most current methods or protocols.
All images are genuine, trustworthy and real standard views of the "before" situation and the long term settled "after" actual results of Dr. Alejandro Nogueira’s work, as well as true intraoperative surgical views and authentic technical or clinical scenarios depicting real practice hands-on cases belonging to Dr. Alejandro Nogueira's skills and expertise.
No other professional but Dr. Alejandro Nogueira himself as leading and executing surgeon has carried out the techniques, procedures and surgeries shown in the galleries.
No images were staged, digitally edited or modified in any way, except for cropping, adjusting and resizing to fit gallery format, removing identifiable elements and blanking with anonymity purposes.
The images of results, treatments, techniques and clinical situations are mere guidance examples aiming to help the patients in their decision-making process, providing an average overview of Dr. Alejandro Nogueira's work; no one of them can be considered as an obligation of any particular results nor a commitment for the application of any specific techniques, therefore you should not base your results expectations on them.
Every patient has to be assessed individually in order to establish a customized prognosis of results and design an individual surgical plan, being somehow unpredictable the real final outcome of any procedure as well the surgical gestures applied during the intervention, since they will depend on multiple particular, frequently unpredictable and sometimes uncontrollable factors.
Even when you feel that you look very similar to another patient in their images, your results will likely vary significantly, because you are a unique person and every individual has not only a completely unique physique, but also uniquely individualistic body healing capacities, scarring tendencies and recovery processes, some of which are unpredictable even in very-healthy patients who rest adequately and do all the other right and prescribed things before and after their procedure.
Previous successful results of a physician do not guarantee future successful procedures and patient's satisfaction.
The images may display content that is graphic in nature showing explicit surgery, clinical events and that may depict partial or total nudity; if you find such material offensive or you are sensitive to it you should not use this feature and should exercise caution before accessing other explicit features of the website.
The images are appropriate for a mature-only audience; if you are under the age of 18 you should not view the content of this website.
All the prices and quotations visible on our website belong to or are calculated out of the reduced price list and do already enjoy by default a -20% discount from the standard price list for our treatments as compensating remuneration for the release and transfer of the intellectual property, the rights of image, the medical records and the personal data of our patients for scientific dissemination, medical teaching, public communication, commercial promotion, advertising marketing, commercial exploitation and disclosure in general, unless they express the opposite at their surgery day booking by opting for the standard prices.
READ MORE ABOUT BENEFITS OF THE COLLABORATIVE MODEL
Our prices are quotations valid for the majority of cases operated on; notwithstanding a few cases are non standard, atypical, requiring exceptional resources and, therefore, needing customized quote calculation; do seek the advice of our Medical and Sales Teams to find out whether your case lies within the standard protocol of management, which actually is the most likely scenario.
Standard quotations do cover the planned protocol of management, including preoperative consultation with the surgeon, preanesthesia examination, basic preoperative tests, surgeon, anesthetist and assistant fees, planned operating room, rental time, regular intraoperative surgical supplies (materials, drugs, etc.), agreed implants (breast, etc.), one recommended postoperative garment (brassiere, corset, etc.), 1 hour recovery unit stay, individual ward room, regular hospital supplies (materials, drugs, etc.) and postoperative office-based care.
Not included in standard quotations are, among others, non basic preoperative tests, pre and postoperative consultant referrals for assessment, additional garments, non hospital supplies (materials, drugs, etc.), postoperative tests and any kind of postoperative re-interventions, postoperative medical or surgical emergencies and costs exceeding the planned protocol of management like unplanned, unforeseeable and unavoidable extended surgical time rental of the operating room, extended hospital stay in standard ward or Intensive Care Unit (ICU) room and all the associated costs with any hospital-based assistance of complications, medicalized repatriation, hostelry accommodation, maintenance and travel costs; we do not take account of any costs not within the scheduled treatment pre and postoperative planned and agreed management.
We do not offer trip packages; the patient is bound to organize and pay for any trip, accommodation, food, transport, etc.
Prices do include the V.A.T.
Prices do not include any kind of travel or revision insurance; do read about the Surgery Shield for revision surgery here should you wish to be covered in such a case.
Treatments are payable in Euros only; we do not accept other currencies as payment of the treatments.
Any currency conversion is non accurate and has indicative purposes only.
Combo Specials discounts are percentages of reduction applied on the retail price of the standard quotations for the treatments of the price list; these discounts are not applicable on non standard cases, customized quotations and charges not included in the standard quotations.
The treatments Breast implants custom XL or Breast reconstruction autologous and the Surgery Shield for any body area treament is expressly excluded from any price reduction, discount and promotion, among them the Combo Specials.
Combo Specials are applied and calculated for each purchase of treatments to be performed simultaneously; Combo Specials are not allowed on treatments to be performed in different anesthetic procedures or different surgical episodes; any given purchase of treatments to be performed simultaneously may include more than one Combo Special.
One given treatment cannot be affected by more than one discount, be it Combo Specials or other discounts; in the event of a conflict due to the coincidence of more than one Combo Specials discount affecting a given treatment, the discount that produces the greatest gross discount in favor of the patient calculated at the given treatment in conflict level will be applied.
The marbellia's General Combo Special only applies to treatments other than those affected by treatment-specific Combo Specials at any given purchase of treatments to be performed simultaneously; for the calculation of the marbellia's General Combo Special all the treatments affected by treatment-specific Combo Specials are considered a single treatment.
Any urgent matter of medical or commercial kind must be addressed through our Telephone Assistance which is operative 24/7/365 to contact with the Medical Team or through our Telephone Support which is available in office hours to contact with the Sales Team.
Priority but non urgent medical or commercial assistance is available by selecting priority option in the corresponding Online Consultation or Customer Support form.
Non urgent and non priority medical consultations may be carried out using the regular Online Consultation or Customer Support form without priority selection.
Due to the competitiveness scenario of the markets most plastic surgery clinics and plastic surgeons feel forced to invest large sums of money into advertising and marketing campaigns; this non medical additional cost is always and necessarily charged on top of the final price paid by patients, leading thus to an overprice of surgeries and treatments. No one patient wishes to bear that financial burden embedded in the surgical costs, furthermore neither surgeons nor clinics are happy to increase their retail prices and penalize their customers with costs not bringing any kind of special medical benefit, safety enhancements or results improvement; the promotion budget aims only to disseminate the public knowledge of a services provider and raise the awareness about its presence to potential customers, but not to make the service or the product a better one.
Seems like this model is a no-way-out labyrinth from which no one can be freed, furthermore it is such a tempting, easy and hassle-free way that actually most patients and plastic surgery providers are locked into it, happily or with resignation, paying a high price due to being non collaborative; however there is an ideal alternative, based on keeping up a good hard work based on a strive for providing quality service and achieving patients' satisfaction, which necessarily requires the decided support of the clients and somehow their involvement in such virtuous business model grounded on top-notch results
READ ABOUT BENEFITS OF THE COLLABORATIVE MODEL
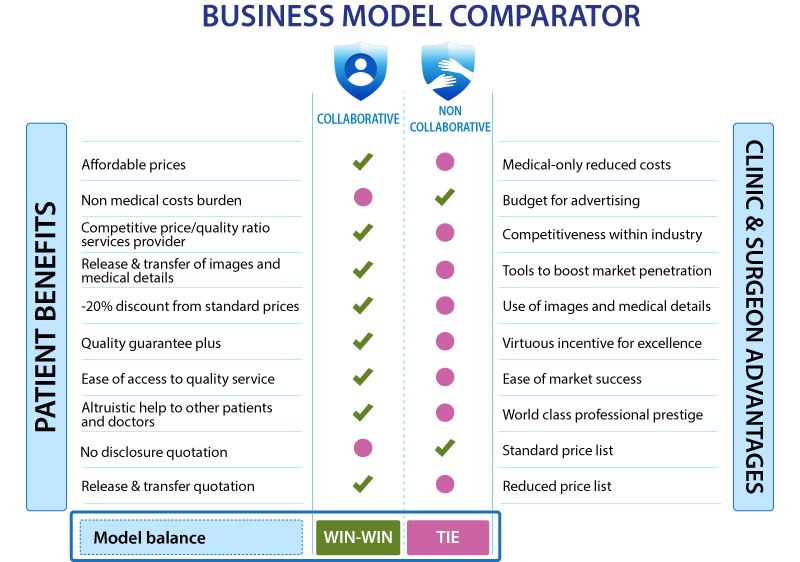
When plastic surgery providers and patients do actively engage into a collaborative economy scenario a win-win basis is set for their relationship, since the clinics and surgeons obtain the best promotion ever possible with no budget for marketing investment and the patients get in return rid of any additional and unnecessary costs; such a price reduction does not represent any loss in the quality of the treatment they are receiving, furthermore this saving achieved will actually reward customers with a reinforced confidence and guarantee the service providers will strive to perform the best job possible and obtain results second to none.
It is not a paradox or contradiction; under a collaborative economy umbrella plastic surgery patients enjoy a greater plus of confidence that clinics and surgeons will do their very best and beyond to satisfy their customers, in spite the price is lower than in marketing-based non collaborative models; plastic surgery providers who found their business sustainability on the pillars of exclusively or mainly incremental budget investment in ongoing promotion campaigns do have little incentive in achieving first-class results and the best patient experiences, since their business model is not based on returning patients after word-of-mouth dissemination of their reputation but on the attraction of cold clients with sophisticated advertising methods of higher or lesser moral acceptability, attracting customers as parachutists randomly landing on unknown land, which is a perverse business model frequently leading to an unavoidable degradation of safety and results quality besides an uncontrollable increase in costs and prices; this marketing-based model creates no incentives to keep up the good work and pushes the prices higher on and on due to require increasing promotional investments.
On the other side, which is definitely our side, clinics and surgeons who rely solely or mostly their existence and survival in the competitive plastic surgery market enjoying the widespread of their excellence extended by their own patients results and satisfaction, like a mill driven by the winds of prestige, have the strongest ever incentive to be the best service providers around, sourced from the support of happy clients and their operated cases as proof of their excellent jobs; needless to say such supporters, the patients, have to enjoy a share of this benefit so that the incentive is reciprocal; under this scenario clinics and surgeons strive to provide the best service and accordingly patients release and transfer in a fair exchange the materials and tools required to build a marketing-budget-free and virtuous business model which creates the perfect incentives to build the best sponsorship-free reputation, based on the grounds of medical quality thus allowing prices control within affordability thanks to the minimal cost of its maintenance.
This is the deal; patients give in our favor the release and transfer of the intellectual property, the rights of image, the medical records and the personal data of their cases for scientific dissemination, medical teaching, public communication, commercial promotion, advertising marketing, commercial exploitation and disclosure in general, and they receive in exchange a compensating remuneration of a -20% discount from the standard price list for our treatments, as it is publicly visible by default in all the prices and quotations on our website.
As can be observed our visible prices are highly competitive if compared with other plastic surgery providers, actually the difference is approximately a -20% from the average price of each particular treatment in other clinics and surgeons from similar economical areas and countries of comparable development; this is not due to any quality or safety downgrading but to our collaborative business model; in other words, the budget which theoretically should be invested in marketing and promotion campaigns is discounted from the retail prices and, unlike other plastic surgery providers, is not wasted into pointless advertising to patients which entails no kind of added value for them; such campaigns are replaced with our superb results publicized thanks our patients support by letting us use their cases' Before & After and Intraoperative & Technical images and medical details; this explains that price gap between us and other clinics and surgeons.
READ LESS ABOUT BENEFITS OF THE COLLABORATIVE MODEL
MODEL KEYNOTES
Patients gain a highly affordable pricing model with yet world-class standards of medical practice, safety and results, and we gain competitiveness within the industry by means of saving the budget theoretically bound to be wasted in marketing.
Patients contribute with their images and medical details and we compensate them with a -20% discount from the expectable average price quoted by comparable clinics and surgeons.
We receive a boost of unbeatable promotion and market penetration by using our awesome operated cases and the patients enjoy a plus of guarantee that we will strive to conduct ourselves to the highest level of excellence and obtain results better than one can imagine.
We help you access the best plastic surgery results and you help us win the race of the market.
Should you feel not interested in collaborating with our business model and still wish to be our patient? No worries, this perfectly possible under the same philosophy of professionalism, devotion and quality, you have to simply express your opposition at surgery day booking by opting for the standard prices and thus give up the -20% discount of the collaborative model, budget which will be used to promote our business in sponsorships, campaigns or one-time actions aiming to attract new customers who, without your help to take the right decision for their surgery, may need sponsored channels to know about us.
Keep in mind that taking part in our collaborative business model is also an altruist way to help other prospective patients to find the medically right and commercially suitable plastic surgery provider, besides collaborating in the medical education of other surgeons and medical professionals.
We offer a flexible consumer-to-business relationship by letting our patients choose between a release & transfer quotation model in which the standard price list receives a -20% discount becoming thus the reduced price list, and a no disclosure quotation in which the standard price list applies and the patient misses such compensating remuneration.
Two models under the same quality involving different prices and marketing-building strategies; you receive always one guarantee: our commitment we will give you our best.
You attempted an unauthorized action. All contents of this site are private and protected. Print screen are not allowed. We have reported with your data location to prevent any ilegal action against the protected contents of this website.









 Sending vote...
Sending vote...

 READ MORE ABOUT BENEFITS OF THE COLLABORATIVE MODEL
READ MORE ABOUT BENEFITS OF THE COLLABORATIVE MODEL
 +34-900-838448
+34-900-838448 +44-0-800-0488400
+44-0-800-0488400 +1-844-4000840
+1-844-4000840























































































































































































































































































































































































































































